| Feature | Brain MRI | Brain CT Scan |
|---|---|---|
| Detail (Soft Tissue) | High (30-40 tissue gradations) | Lower (4-5 gradations) |
| Radiation | None | Ionizing Radiation |
| Scan Time | 30-45 Minutes | ~5 Minutes |
| Best For... | MS, Tumors, Small Strokes | Acute Trauma, Bone Fractures |
How the Technology Actually Works
To understand your results, you first need to know that an MRI isn't just one picture; it's a series of different "sequences." Think of these as different filters on a camera, each designed to make a specific type of tissue stand out. First, there is T1-weighted imaging. In this view, fat looks bright and water (like the fluid in your brain) looks dark. Radiologists use this mostly for anatomy-basically, to see if the brain's structure is shaped correctly. Then there is T2-weighted imaging. Here, water and fluid are bright. Since most brain injuries or diseases cause swelling (edema), T2 images make these problem areas "glow," making them easier to spot. However, because normal cerebrospinal fluid (CSF) is also bright, it can sometimes hide a lesion. That's where FLAIR (Fluid-Attenuated Inversion Recovery) comes in. FLAIR is a clever version of T2 that "turns off" the signal from the normal fluid. If you see a bright spot on a FLAIR image, it's usually not normal fluid-it's likely pathology, such as a plaque from multiple sclerosis. This sequence is the MVP for detecting inflammation and chronic lesions.Spotting Acute Issues: Stroke and Bleeding
When a doctor suspects a stroke, they don't use T1 or T2; they go straight to diffusion-weighted imaging (DWI). This is an incredibly sensitive tool that detects restricted water movement in the brain. In a healthy brain, water molecules move freely. But when a stroke happens, cells swell and trap water. DWI can pick up this change within 30 minutes of a stroke starting. In contrast, a CT scan might not show any one-time changes for 6 to 24 hours. This speed is a matter of life and death, as it tells doctors exactly when to administer clot-busting drugs. For bleeding, specialists use susceptibility-weighted imaging (SWI). This sequence is hypersensitive to iron. Since blood contains iron (hemosiderin), SWI can find tiny "microbleeds" that are almost invisible on other scans. It's often used to check for old trauma or complications from high blood pressure.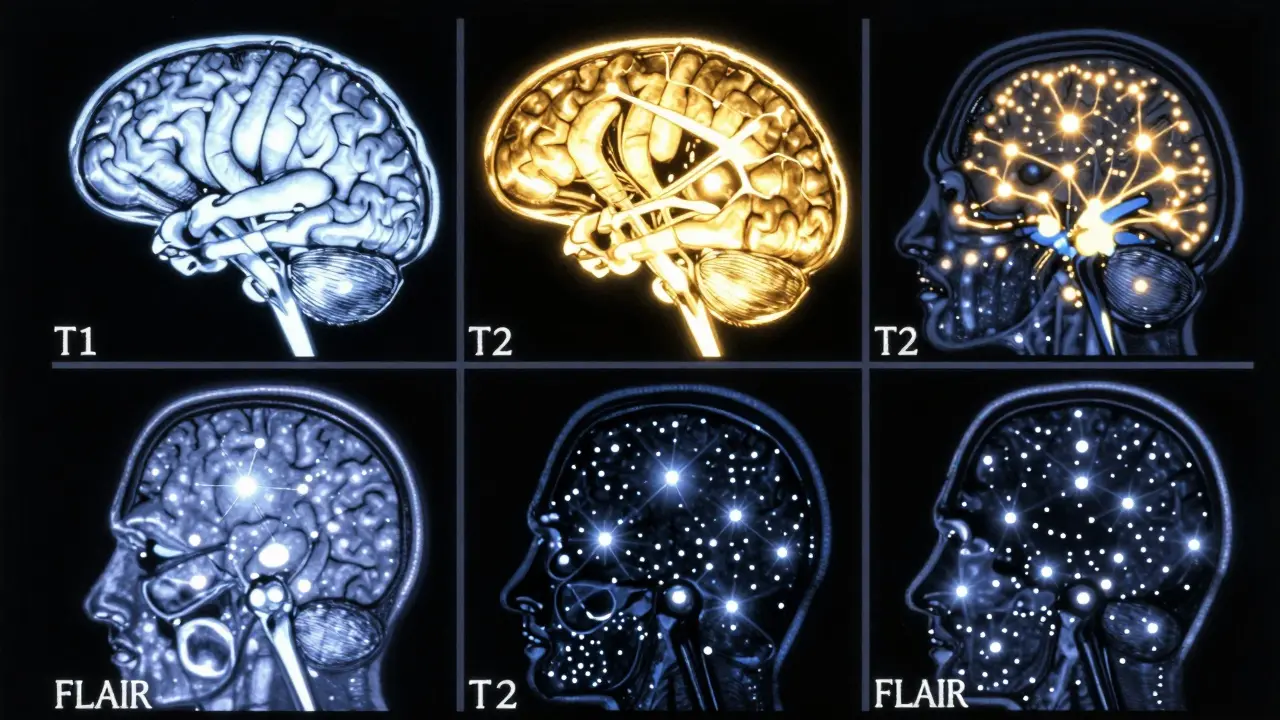
Common Findings and What They Mean
If you're reading your report and see the word "hyperintensity," don't panic. It simply means an area that looks brighter than it should. However, the meaning depends entirely on where that spot is located. For example, small bright spots in the basal ganglia (the deep center of the brain) are often just old "lacunar infarctions"-tiny, silent strokes that many people have as they age and aren't even aware of. On the other hand, if those bright spots are located in the periventricular area (around the fluid-filled spaces), they could be signs of inflammation or MS. Another common finding is "cerebral atrophy," which is just a fancy way of saying the brain has shrunk slightly. Radiologists usually check this on FLAIR images. If they used T2 images, the bright fluid filling the extra space might make the brain look more shrunken than it actually is, leading to an overestimation of the atrophy.The Practical Side: What to Expect During Your Scan
An MRI session typically lasts between 30 and 45 minutes. You'll be sliding into a tube that acts as a giant magnet. Because of this, safety is the number one priority. If you have a pacemaker or a cochlear implant, you must tell the staff immediately, as the magnetic field can move or deactivate these devices. Most clinics use either a 1.5T or 3.0T machine. The "T" stands for Tesla, which measures magnetic strength. A 3.0T machine is essentially a more powerful lens; it provides about 40% more signal, allowing doctors to see tiny structures, like the cranial nerves, with much greater clarity. If you're being screened for a very small tumor, like an acoustic neuroma, a 3.0T scan is often the preferred choice.
When Is an MRI Not the Best Choice?
Despite its power, the MRI isn't always the right tool. For one, it's slow. If a patient is unstable or has severe trauma, spending 40 minutes in a tube is dangerous. A CT scan, which takes only five minutes, is far safer and faster for triage. There is also the issue of over-testing. Some doctors warn against getting an MRI for a standard headache without any other neurological symptoms. Studies show that in people with simple headaches, an MRI finds something "abnormal" only about 1.3% of the time. Most of these findings are "incidentalomas"-random quirks of anatomy that don't actually cause any problems but can lead to unnecessary anxiety and more expensive tests.Does an MRI use radiation?
No, unlike CT scans or X-rays, MRIs use powerful magnets and radio waves to create images. There is no ionizing radiation involved, which makes it much safer for children and people who need repeated scans to monitor a condition.
Why is my report mentioning FLAIR and T2?
These are different "settings" on the MRI machine. T2 makes water and swelling look bright. FLAIR is a special version of T2 that hides the normal brain fluid so that only the "bad" bright spots (like lesions or inflammation) remain visible.
Can an MRI detect a stroke immediately?
Yes, specifically using a sequence called Diffusion-Weighted Imaging (DWI). DWI can identify a lack of blood flow to the brain within minutes of the stroke starting, whereas a CT scan might take hours to show the same damage.
What is a 'hyperintensity' on a brain scan?
A hyperintensity is simply an area that appears brighter than the surrounding tissue. Depending on the location and the sequence used, it could be anything from a normal age-related change or a tiny old stroke to an active lesion from multiple sclerosis.
Is 3.0T better than 1.5T?
Generally, yes. A 3.0T MRI has a stronger magnetic field, which provides a higher signal-to-noise ratio. This means the images are crisper and it's easier for radiologists to spot very small abnormalities, such as tiny tumors in the auditory canal.